
For more, see A. Kenneth Wuertenberg’s companion article on the impact of the Olmstead decision on community mental health.
by Kathleen Brian
On Thursday, May 4, 2017, the U.S. House of Representatives voted to pass the American Health Care Act (AHCA). Despite the guise of free market equilibrium and individual choice, in themselves concepts that have spurred remarkably robust critiques, the text’s design and belabored passage was intended to repeal and recast the Patient Protection and Affordable Care Act (ACA). The exodus of major insurers, as well as states’ scramble for Medicaid waivers, began immediately. Meanwhile, mental health advocates called foul: the plan as passed would viciously undermine those aspects of the ACA most identified with significant gains in the realm of insurance equity for mental health care and substance abuse treatment.
Though far from perfect, the ACA, in conjunction with the subsequent Health Care & Education Reconciliation Act (2010), represented the culmination of a decades-long effort to secure equal coverage for mental health, substance abuse, and behavioral health treatment.[1] It established minimum policy standards for mental health care, in part by defining it as an essential health benefit. It eliminated payment limits and exclusions based in pre-existing conditions which disproportionately targeted individuals with mental disabilities. It expanded the number of qualified individuals with access to mental health services under the rubric of Medicaid and created new possibilities for home- and community-based mental health care.[2]

The newly-minted AHCA would, in effect, nullify these successes. Atop these targeted dismantlings, the AHCA layered new stipulations for the creation of high-risk pools for individuals with pre-existing conditions, as well as Medicaid rollbacks through the capacious potential for state exemptions, and the redefinition of essential health benefits.[3] Simply put, people with mental disabilities are poised to experience significant, disruptive, and deadly setbacks in the realm of access.
Our contemporary landscape thus suggests a flare-up of an actual pre-existing condition for disabled citizens and those non-disabled citizens who advocate alongside them: unequal access to insurance coverage.
Since the 1990s, advocates of mental health parity have increasingly focused on both the state and federal levels. They also have increasingly articulated their demands for equitable coverage through appeals to anti-discrimination oversight, citing the extent to which, historically speaking, the healthcare requirements of people with mental disabilities have been marginalized or excluded. That private insurance companies would not bear financial responsibility for mental health care, they reminded policy makers, was neither natural nor inevitable.[4] Equal access to care, in other words, became a civil rights issue. And if federal legislation is any indication, the strategy was a successful one: the ACA was preceded by, and extended key provisions in, the Mental Health Equitable Treatment Act of 2001 (MHET) and the Mental Health Parity and Substance Abuse Equity Act of 2008 (MHPSAE).
Until we are willing to imagine the unimaginable—namely, the provision of care without insurance as intermediary—we will remain captives to this economic model of wellbeing.
Despite this shift in framework, however, and despite this apparent progress, the economic interests of the insurance industry, yoked to the economic interests of the elite, continue to set the terms of the debate: the healthcare requirements of people with mental disabilities seem unspeakable beyond the realm of the economic. Indeed, demands for mental health parity remain captives of an economic model of wellbeing that resulted, in no small degree, from the insatiability of the insurance industry. I want to suggest, then, that any conversation about health care must begin with the collective acknowledgement of a simple fact: the selective incorporation of humans based on statistical predictions of vitality is the foundation upon which insurance companies assembled themselves. The very essence of the industry was (and is) the development of exclusions, based in statistical imaginings, that would swell corporate profit. Until we are willing to imagine the unimaginable—namely, the provision of care without insurance as intermediary—we will remain captives to this economic model of wellbeing. And a crucial first step toward imagining such alternative possibilities is to remind ourselves of the remarkably recent creation of this pernicious and dangerously biopolitical model.
* * *
It was by no means inevitable that we would come to think of wellbeing in financial terms, or that, within this framework, insurance companies would cast mental disabilities and substance dependency as pre-existing conditions that justified exclusion from benefits and higher premiums. Some have hazarded explanations for how this came to be: insurance coverage for the healthcare needs of people with mental disabilities, the story goes, was something of an afterthought, a problem that did not present itself with any force until the second half of the twentieth century. This was reasonable, by and large, because people with mental disabilities received medical care under the broad rubric of public, residential institutions, regardless of whether said institution was nominally educational, therapeutic, custodial, or carceral.[5] We could pose a number of critiques in response to this standard narrative, not last of all that many people with mental disabilities were unable to access adequate care, mental or physical, under the state-run system.
We might also, though, question the assumption that insurers were generally unconcerned with mental disability. We might ask instead what insurance underwriters thought about mental disabilities, and how these ideas contributed to baseline exclusionary strategies within the industry.[6]
In the United States, the commercial life insurance industry became a significant presence in the middle third of the nineteenth century. This industry, in turn, spawned the industrial, accident, and health insurance industries in the late-nineteenth- and early-twentieth centuries. It took roughly a century for the insurance model to claw its way to its present central position within the healthcare system.[7] The infancy of the commercial life insurance, then, exposes the economic model of wellbeing in the making, and understand the exclusion of people with mental disabilities.

The notion that an individual would send regular payments to a corporation, the officers of which, according to a pre-arranged contract, would hold the money and distribute it to third party recipients in cases of illness or death, only gained significant traction in the antebellum period.[8] Even then, it did not convince a majority. Rather, it was the purview, by and large, of the urban white middle classes. Early insurance policies excluded death by suicide in order to maximize profits by minimizing risk.[9] In their efforts to partition humans into “good risks” and “bad risks,” companies attended to general healthfulness, but also refused to insure individuals who held certain jobs, or who lived in—or traveled to—purportedly dangerous places. Mining and sailoring, for example, often meant automatic disqualification, while travel to the South and the Pacific Northwest—considered particularly treacherous – was also excluded.[10]
It was simple enough to determine whether a person lived in Alabama or worked with explosives. Sniffing out an applicant’s daily doings and habits of health, though, could be trickier. The industry’s initial answer to this was to expand its agency system, which allowed companies to rely on an insurance agent’s local knowledge and proximate access to applicants to verify or refute a medical certification sent along by a local practitioner. It was not unheard of, after all, for a family doctor to fib a little, or to minimize a condition, in order to secure coverage for a friend or long-time patient. In fact, insurance companies soon decided to circumvent the intimacy of the doctor-patient relationship by including doctors on their payroll—doctors specifically tasked with excavating the “real” health status of an applicant over and against the applicant’s own claims. Whether uncovered by an agent or a medical examiner, for example, an observed “habit of intemperance”—later known as alcoholism—typically meant automatic rejection. Though they varied slightly from company to company, and from policy to policy, conditions of exclusion were always detailed, precise, and indicated exactly who the insurance companies wanted to insure: young, temperate, non-disabled men who populated the urbanizing, industrializing northeast.
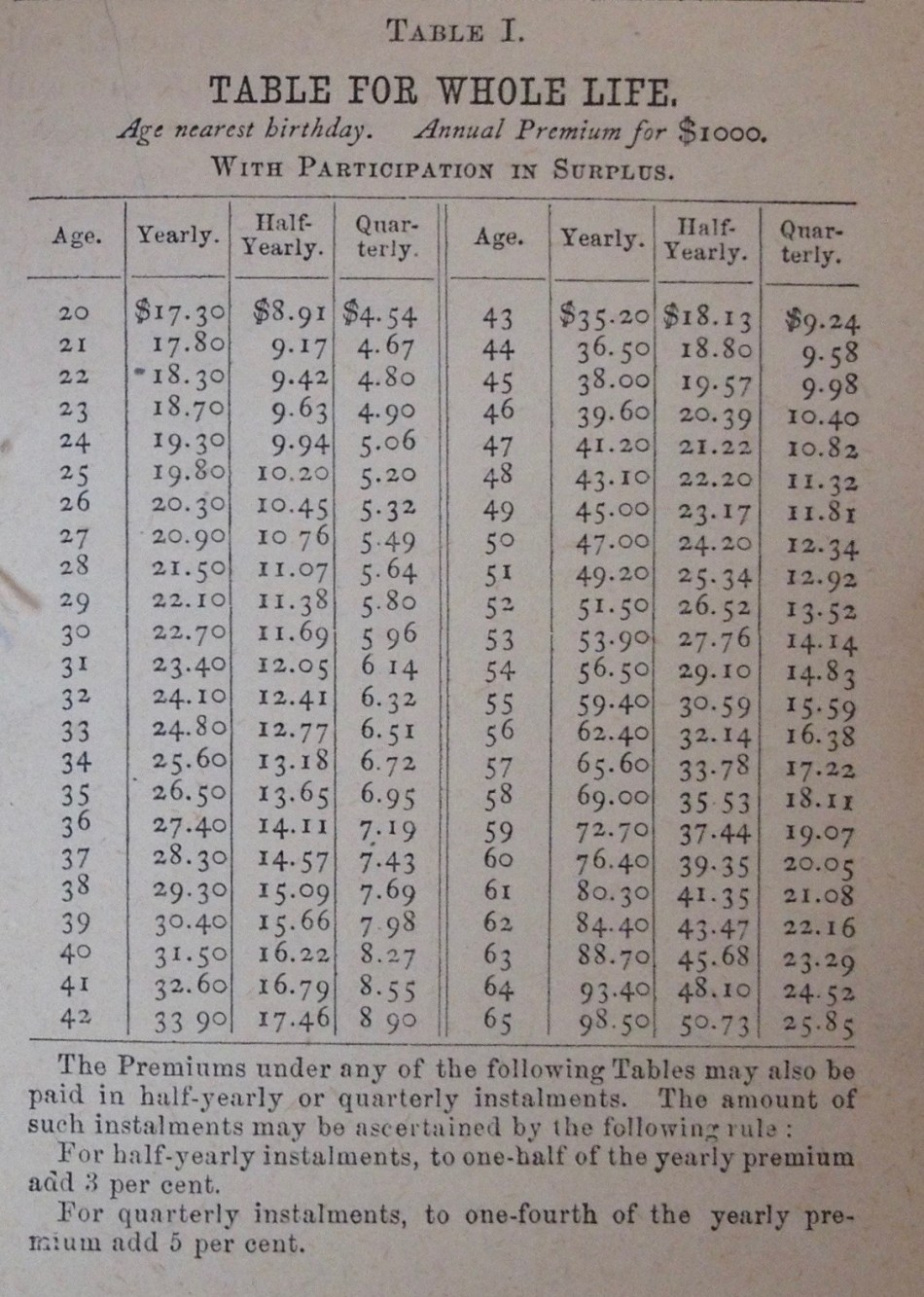
It does not take much to imagine company men imagining just how long such men would pay into the company without demanding remuneration. And as the insurance industry grew over the middle third of the nineteenth century, so, too, did the financial interest in elongating life and predicting death. New studious alliances among medical, legal, and insurance professionals emerged. They developed studies of mortality and disease morbidity that sometimes relied on data generated by the state, while others drew on the statistical findings of the companies themselves. The formation of a discreet insurance public after 1852, which allowed insurance advocates to compare notes, strategize, and perfect exclusionary practices, also facilitated new knowledge networks and intercompany alliances that one contemporary termed “the insurance fraternity.”[11]
Insurers announced the development of an intercompany register in 1878, which revolutionized the industry. It contained the names of every person who had applied to participating companies for a policy of life insurance, with “especial reference to those persons who are found to be unfit subjects.”[12] The registry, which began as a network of twenty companies, was to be circulated each week to guard against people who, having been rejected by one insurance underwriter, “at once report to another company, who, from carelessness on the part of their medical officer or other causes, grant a policy only to find in short time that they have made a mistake.”[13] The systematic development of exclusions based on pre-existing conditions, in other words, was well underway.
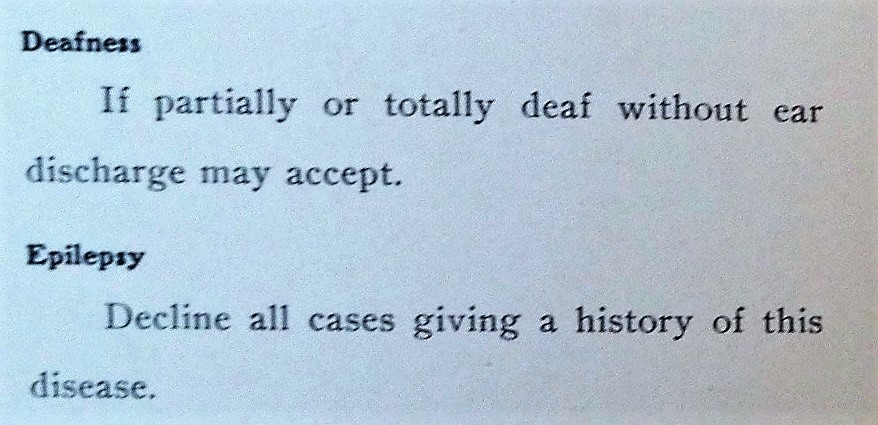
Two other developments of the second half of the century bore significantly on how insurance companies related to people with mental disabilities, and both were encapsulated in the industry’s evolving attitude toward suicide. On the one hand, insurers were increasingly concerned about connections between insanity and the increasingly solidified connection between insanity and self-harm. They were also, at the same time, increasingly drawn to hereditary explanations of mental disabilities.
In the case of commercial life insurance, these phenomena were deeply connected. In the period immediately following the Civil War, insurance companies found themselves increasingly embroiled in what one termed the “suicide contests,” or legal battles over whether or not a company had the right to refuse policy payouts in cases of suicide. Insurers tried to guard against paying beneficiaries in such cases. The majority included stipulation in their policies to the effect that, when death occurred as a result of “one’s own hand,” the company was not liable—stipulations colloquially referred to as the “suicide clause.”[14]
At its most fundamental, the story of this legal warfare is one of escalating attempts by beneficiaries and insurance companies to guarantee their own economic interests. The proliferation of suits, however, had a secondary affect, as well, not least of all because companies kept losing. Of 243 decisions between 1843 and 1900, 69 percent were decided in favor of the beneficiaries. These losses led to companies to pursue with growing zeal the family history, the chronicity of certain diagnoses, and the claim that “a suicidal tendency was eminently heritable.” [15] Medical and actuarial studies proliferated as a way to “prove” these claims and, in turn, justify benefits exclusion.

By the final decades of the nineteenth century, then, the practice of pre-policy exclusions for a majority of people with mental disabilities—but especially those whose families carried the “taint” of suicide—had become commonplace commonsense. In an 1880 treatise on effective examinations of policy applicants, for example, J. Adams Allen instructed medical examiners that although insanity did not always “tend to shorten life directly,” its presence, even when “incipient or masked,” should serve as an automatic disqualification.[16] So when asylum physician and superintendent Robert Jones wrote in 1905 that “insanity per se is inimical to life,” few in the insurance industry would have been surprised.[17] The exclusion of people with mental disabilities was a crucial foundation upon which the insurance industry constructed itself. It was central to their business model.
It was not until the 1930s and 1940s, when confronting the rising cost of medical care that resulted from the insurance company model, that reformers reversed this emphasis and began actively to imagine insurance as a primary financial facilitator of care.
This, of course, was the same historical moment in which debates about universal or compulsory health insurance became increasingly cacophonous, incorporating, among others, the voices of government officials and politicians, unions and labor activists, medical and legal professionals, academics and social reformers. Early demands stressed remuneration for lost wages over remuneration for medical care. It was not until the 1930s and 1940s, when confronting the rising cost of medical care that resulted from the insurance company model, that reformers reversed this emphasis and began actively to imagine insurance as a primary financial facilitator of care. It was also during these decades that the insurance model, with the dogged support of the American Medical Association (AMA), ascended to dominance and, in the scramble to prove their own efficacy, expanded general coverage.[18]
At that point, however, the insurance industry had made the systematic exclusion of people with mental disabilities an everyday doing for more than a half-century. For insurance companies, the economic model of wellbeing that allowed them to prosper was quite simple: avoid underwriting these people.
* * *
The most pressing pre-existing condition for our contemporary debates about healthcare is one that, far too often, goes unarticulated: private insurance companies only become viable through systematic exclusion. Their own longevity is dependent upon their statistical imaginings of the longevity of others. Since the late nineteenth century, they have worked very hard to imagine people with mental disabilities as inherently, immutably less vital.
Conversations around mental health care and substance abuse treatment, not to mention the other healthcare requirements of people with mental disabilities, must be informed by this history. Perhaps then they will be able to venture beyond—or, better yet, before—the economic model of wellbeing with all the irreverence of the economically indefensible. As Ben Feldman has recently suggested, and as so many unlikely reformers have in the past, we need to “demand the ‘impossible’ until it is impossible no longer.” It is time to grapple with that which has been designated unworkable, improbable, and unthinkable: the provision of healthcare for its own sake, without the parasitic presence of insurance companies.

Kathleen Brian teaches in the Liberal Studies Department at Western Washington University. She is a cultural and intellectual historian who specializes in histories of science, medicine, and public health in the United States and its imperial outposts, as well as critical race and disability theory. Her work has appeared in the Bulletin of the History of Medicine and the Journal of Literary and Cultural Disability Studies, among others, and her co-edited collection, Phallacies: Historical Intersections of Disability and Masculinity, is forthcoming from Oxford University Press (2017). She is currently at work on a book project that rethinks the origins and agendas of American eugenics through the history of suicide. She can be contacted at kathleen.brian@wwu.edu.
* * *
Our collected volume of essays, Demand the Impossible: Essays in History As Activism, is now available on Amazon! Based on research first featured on The Activist History Review, the twelve essays in this volume examine the role of history in shaping ongoing debates over monuments, racism, clean energy, health care, poverty, and the Democratic Party. Together they show the ways that the issues of today are historical expressions of power that continue to shape the present. Also, be sure to review our book on Goodreads and join our Goodreads group to receive notifications about upcoming promotions and book discussions for Demand the Impossible!
* * *
We here at The Activist History Review are always working to expand and develop our mission, vision, and goals for the future. These efforts sometimes necessitate a budget slightly larger than our own pockets. If you have enjoyed reading the content we host here on the site, please consider donating to our cause.
![]()
Notes
[1] On this history, see Colleen L. Barry, Haiden A. Huskamp, and Howard Goldman, “A Political History of Federal Mental Health and Addiction Insurance Parity,” The Milbank Quarterly 88.3 (2010): 404-433; Richard G. Frank, Chris Koyanagi, and Thomas C. McGuire, “The Politics and Economics of Mental Health ‘Parity’ Laws,” Heath Affairs 16.4 (July/August 1997): 108-119; Gerald Grob and Howard H. Goldman, The Dilemma of Federal Mental Health Policy: Radical Reform or Incremental Change? (New Brunswick, NJ: Rutgers University Press, 2006); and Thomas C. McGuire, Financing Psychotherapy: Costs, Effects, and Public Policy (Cambridge, MA: Ballinger Pub. Co., 1981).
[2] “Health Care Reform,” Judge David L. Bazelon Center for Mental Health Law, available at http://www.bazelon.org/Where-We-Stand/Access-to-Services/Health-Care-Reform.aspx (accessed 11 May 2017); “Insurance Market Reforms in the Patient Protection & Affordable Care Act and the Health Care & Education Reconciliation Act, Judge David L. Bazelon Center for Mental Health Law, available at http://www.bazelon.org/LinkClick.aspx?fileticket=4SLhcBf-V7o%3D&tabid=137 (accessed 11 May 2017).
[3] See especially “Title I,” which rolls back the successes established in the ACA; “Title II, Sec. 232,” which addresses Medicaid; and “Title III, Sec. 301, Subtitle B,” and “Title III, Sec. 311,” which creates high-risk pools for individuals with pre-existing conditions. American Health Care Act, H.R. 277, 115th Cong. (2017), at https://www.congress.gov/115/bills/hr277/BILLS-115hr277ih.pdf (accessed 10 May 2017).
[4] Barry, Huskamp, and Goldman, “A Political History of Parity,” 409-411.
[5] Some have argued that the zealous insurance reformers of the 1930s, perpetuating the long-established understanding of mental health care as a state concern, emphasized state legislatures that had the power to mandate minimum benefit levels for certain psychiatric diagnoses and substance abuse disorders. As a result, the more equitable coverage of mental health care only became an urgent question in the period of deinstitutionalization, which began in earnest in the mid-1950s and accelerated across subsequent decades. It was not until the 1950s that psychiatric services were covered for the insured middle- and upper-classes. See especially Barry, Huskamp, and Goldman, “A Political History of Parity,” 409-411; Grob and Goldman, The Dilemma of Federal Mental Health Policy; and Howard H. Goldman, Steven S. Sharfstein, and Richard G. Frank, “Equity and Parity in Psychiatric Care,” Psychiatric Annals 13.6 (June 1983): 488-491. On the comparative role of psychotropic drugs and federal policy on the process of deinstitutionalization, see William Gronfein, “Psychotropic Drugs and Deinstitutionalization,” Social Problems 32.5 (June 1985): 437-454. Jonathan Metzl’s research exposes the extent to which the racialized and gendered dimensions of this process were obscured by the rhetoric of “criminality. See Jonathan Metzl, The Protest Psychosis: How Schizophrenia Became a Black Disease (Boston: Beacon Press, 2009), especially pp. 139-44 and 175-211.
[6] Most works on the insurance industry do not deal extensively with mental disabilities or with mental health care. See, for example, John E. Murray, Origins of American Health Insurance: A History of Industrial Sickness Funds (New Haven, CT: Yale University Press, 2007); Ronald L. Numbers, ed. Compulsory Health Insurance: The Continuing American Debate (London and Westport, CT: Greenwood Press, 1982). When they do, it is typically in passing and subsumed under more general concerns. See, for example, Christy Ford Chapin, Ensuring America’s Health: The Public Creation of the Corporate Health Care System (New York: Cambridge University Press, 2015), 11, 184, 226; Ronald L. Numbers, Almost Persuaded: American Physicians and Compulsory Health Insurance (Baltimore: The Johns Hopkins University Press, 1978), 76, 5, 2, 7; John Fabian Witt, Crippled Workingmen, Destitute Widows, and the Remaking of American Law (Cambridge, MA: Harvard University Press, 2004), esp. 76-95; and Sharon Ann Murphy, Investing in Life: Insurance in Antebellum America (Baltimore: The Johns Hopkins University Press, 2010), 77-96.
[7] By using this verb, I tentatively position myself in contradistinction to an argument advanced by Christy Chapin, who sees the American Medical Association as, in essence, forcing the hand of the commercial life insurance industry in the late 1930s. See Christy Ford Chapin, Ensuring America’s Health: The Public Creation of the Corporate Health Care System (New York: Cambridge University Press, 2015), esp. 27-33.
[8] The best work on industry strategies for expansion during this period can be found in business historian Murphy, Investing in Life. Despite the title, Murphy deals extensively with the wartime and postbellum tactics of various companies, arguing that the expansion of industry during the 1860s forced life insurance firms to liberalize policies, spend extensively on various marketing techniques, and participate in the postbellum “speculative frenzy” in order to maintain a competitive footing in the market. In Murphy’s account, the suicide contests emerge only as a cautionary tale of the liberalizing tactics of postbellum companies. Murphy writes into body of scholarship that attempts to account for the historical processes by which life insurance companies became so incredibly (and suddenly) successful in the 1840s. Early interpretations emphasized economic factors and developments internal to the industry, such as the development of the agency system and other marketing techniques. Particularly successful representations of this school are J. Owen Stalson, Marketing Life Insurance: Its History in America (New York: McGraw Hill, 1969) and Morton Keller, The Life Insurance Enterprise, 1885-1910 (Cambridge, MA: Harvard University Press, 1963). In response to this, cultural historians have emphasized ideological changes such as secularization that made the purchase of life insurance more palatable for middle-class Anglo-Americans. See Viviana A. Zelizer, Morals and Markets: The Development of Life Insurance in the United States (New York: Columbia University Press, 1979). Like Stalson, Murphy underscores the centrality of the agency system; but she argues that the system was important not because it brought a greater number of policy-seekers to the firm but because it allowed agents to evaluate candidates in person, thereby imbuing the physical examination with greater surety and lowering the amount of risk the companies would assume. See Sharon Ann Murphy’s Investing in Life: Insurance in Antebellum America (Baltimore: Johns Hopkins University Press, 2010), 22-23, 175.
[9] “Suicide,” Insurance Monitor Extra 10 (December 1862): 1. The Massachusetts Hospital Life Insurance Company included a suicide clause in the first policy it issued in 1823. See Sharon Ann Murphy, Investing in Life: Insurance in Antebellum America (Baltimore: Johns Hopkins University Press, 2010), 92.
[10] Pennsylvania Mutual Life Insurance Company, “Insurance Policy for Walter Giles,” 28 August 1854, Vertical File 60167, H. Furlong Baldwin Library Special Collections, Maryland Historical Society, Baltimore.
[11] This insurance public began with the commencement of Tuckett’s Insurance Monitor (1852), which was followed by the American Law Register (1852); Insurance Monitor (1853); Life Insurance Advocate (1855); United States Insurance Gazette (1855); Philadelphia Underwriter (1857); American Life Assurance Magazine and Journal of Actuaries (1859); American Exchange and Review (1862); Baltimore Underwriter (1865); American Law Review (1866); Day’s Insurance Messenger (1867); Digest of Insurance Law in the United States (1867); Our Mutual Friend (1867); Aetna (1868); Insurance Times (1868); Mutual Benefit Life Insurance Advocate (1868); New York Newsletter (1868); Spectator (1868); Hahnemannian (1869); Union Central Advocate (1869); Journal of the Mutual Life Association of Virginia (1870); Minnesota Atlas (1870); Agent (1870); Oak Leaf (1870); and the Insurance Law Journal (1871).
[12] “A LIFE INSURANCE COMBINATION. REGISTERING REJECTED APPLICANTS,” American Life Assurance Magazine and Journal of Actuaries 19 (1878): 91.
[13] Ibid., The twenty companies involved initially were the New York Life Insurance Company; National Company (Washington); National Life (Montpelier); Northwestern (Milwaukee); Mutual Life (Philadelphia); Phoenix (Hartford); Union Central (Cincinnati); Provident (New York); Aetna (Hartford, Berkshire, Pittsfield); Brooklyn Company (New York); Mutual and General (Hartford); Germania (New York); Continental (Hartford); Globe (New York); Home (New York); Hartford Life and Accident (Hartford); Knickerbocker (New York); Manhattan (New York); Mutual (Springfield, MA); and John Hancock Life (Boston).
[14] “The Suicide Risk,” New York Observer and Chronicle, 17 June 1875, as reprinted from the Philadelphia Observer. The Observer also noted that the Philadelphia Ledger remarked that “the general adverse results” of the contests would “some time or other make it necessary for the underwriters to devise some new form for that clause in their policies.”
[15] “Life Assurance Medical Officers Association: Insanity and Epilepsy in Relation to Life Assurance,” Lancet (10 December 1904): 1656-1657. Quote from p. 1657.
[16] J. Adams Allen, Medical Examinations for Life Insurance, Seventh Edition, Revised and Enlarged (New York and Chicago: The Spectator Company, 1880), 137.
[17] Robert Jones, “Remarks Upon Insanity and Epilepsy in Regard to the Duration of Life,” American Journal of Insanity 61.3 (January 1905): 467-482. Quote appears on p. 481.
[18] Chapin, Ensuring America’s Health, esp. 27-36.


{kind=link}
Pingback: The Olmstead Decision and Community Mental Health – The Activist History Review
Pingback: COVID-19 Shows Republicans’ Commitment to Eugenics – The Activist History Review
Pingback: Eugenics and the White Moderate: Reflections on the COVID Crisis from Reconstruction (Guest Post) | Society for US Intellectual History