
For more, see A. Kenneth Wuertenberg’s examination of the impact of the Olmstead decision on community mental health.
by Jade Shepherd
In 1884, four years after his release from Broadmoor Criminal Lunatic Asylum[1], and following the death of his sister, George Longmore re-admitted himself into the asylum. Afterwards, he wrote to his brother:
“Dear brother me coming to Broadmoor I know has been a sad blow to your feelings. I am sorry for causing you so much pain…I must make the best of it for a time now. I do wish it had never happened on account of my dear wife and my dear mother.
I shall be made as comfortable as can be while here. Dear brother…I must conclude sending my kind love to you which I am sorry for causing so much pain. I hope you will forgive me and please do remember me to dear mother with many kisses and sister Betsy and John and all my friends, so goodbye for the present.
I remain
Your affectionate brother
George Longmore”[2]
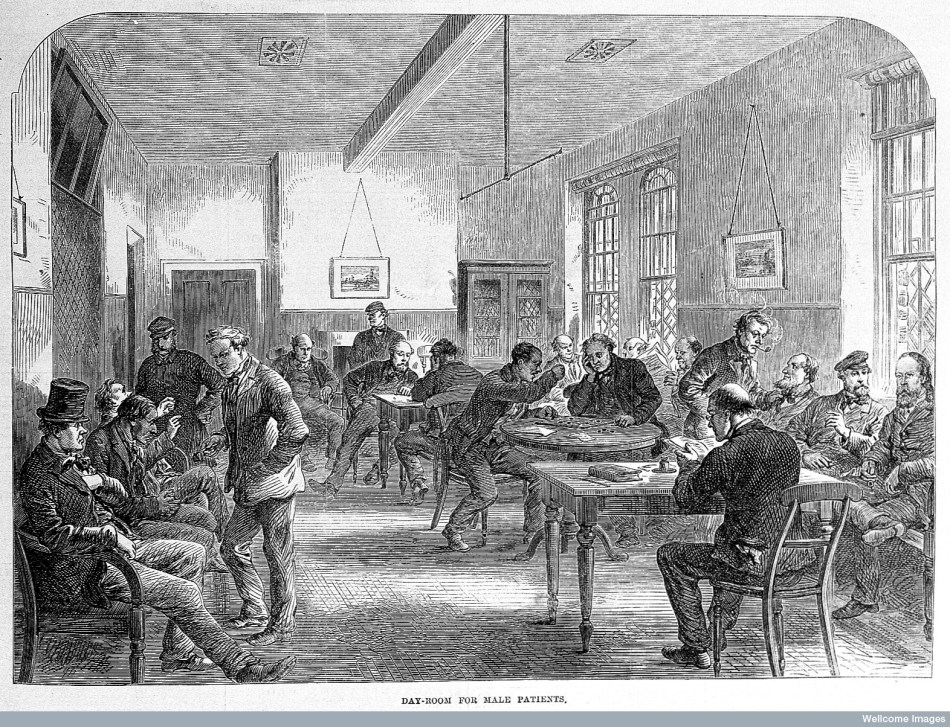
Longmore appears to have been torn between two communities: one familial, and one at Broadmoor. With his family seemingly unable to offer him the care and support he needed, Longmore viewed the asylum as a sanctuary within which he would receive necessary treatment and support. The asylum not only provided medical care, but also a strong social community. Longmore was free to talk with, work, and partake in leisure pursuits alongside other male patients.
Since the old asylum system was dismantled—a process that began in Britain in the 1960s—the communities that some individuals living with mental illness relied upon, both medical and social, have all but disappeared.
While there was a lot wrong with the institutionalized care offered in the nineteenth and twentieth centuries, cases such as Longmore’s alert us to the benefits of specialized institutions for the care and treatment of those living with mental illness, and the importance of the sense of community that these institutions created. Since the old asylum system was dismantled—a process that began in Britain in the 1960s—the communities that some individuals living with mental illness relied upon, both medical and social, have all but disappeared. Care in the Community was designed to replace the old asylums, but amounted to nothing more than “an attractive slogan.” Writing in the 1970s, author PD James described care in the community as “the absence of care in a community still largely resentful or frightened of mental illness.” Since James wrote this, and as Patrick Cockburn recently observed, “not much has changed for the better.” The apparent criminalization of mental illness—with the prison system seemingly replacing psychiatric hospitals—constitutes an avoidable regression to the seventeenth and early eighteenth centuries.
The philosophy of treatment for insanity before the nineteenth century is infamous: chains, bloodletting and purging. The insane were hidden from view, represented as bestial and inherently irrational. From the mid-eighteenth century ideas about insanity began to change, and there was an increasing desire among medical professionals to adopt a new philosophy and treat insanity with so-called moral treatment. Historians have referred to this change as the domestication of insanity. Under moral treatment, the restraint and seclusion of patients was frowned upon, and the importance of kind and patient asylum staff was emphasized, with the superintendent acting as a father figure to patients. Recreations and amusements were promoted as important elements of treatment that would help to divert and heal patients’ minds. These amusements included reading, painting, writing and playing games. Patients were also given religious and secular instruction as part of their treatment, and because moral value was ascribed to work to relieve idleness and prevent patients from dwelling upon their condition, they were encouraged to practice their trade (or learn one).
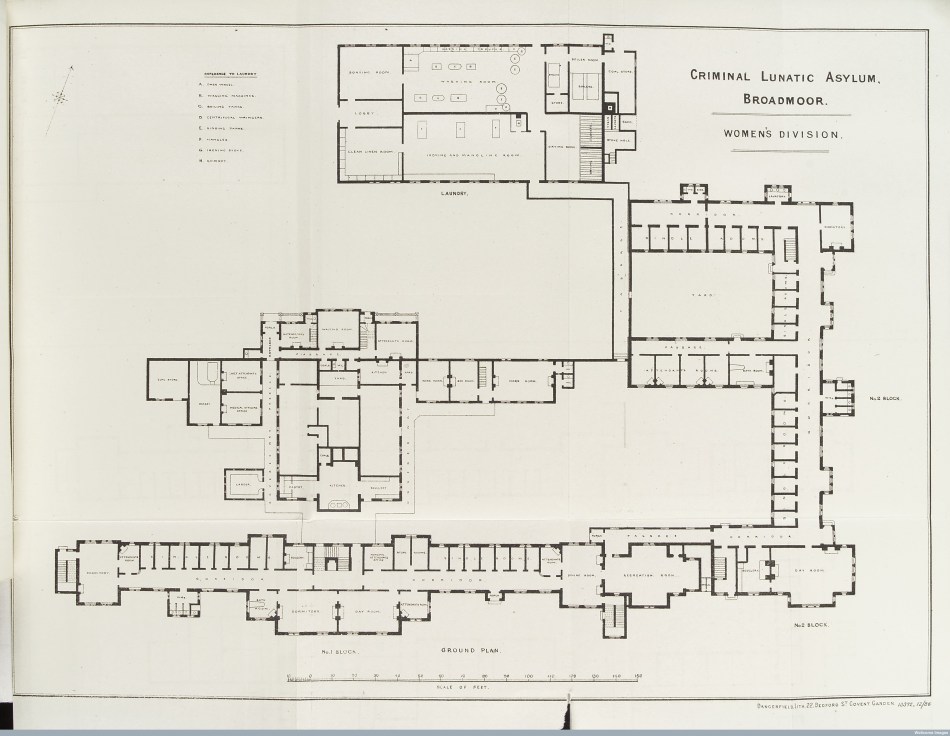
(1887). Courtesy of Wellcome Library and Creative Commons.
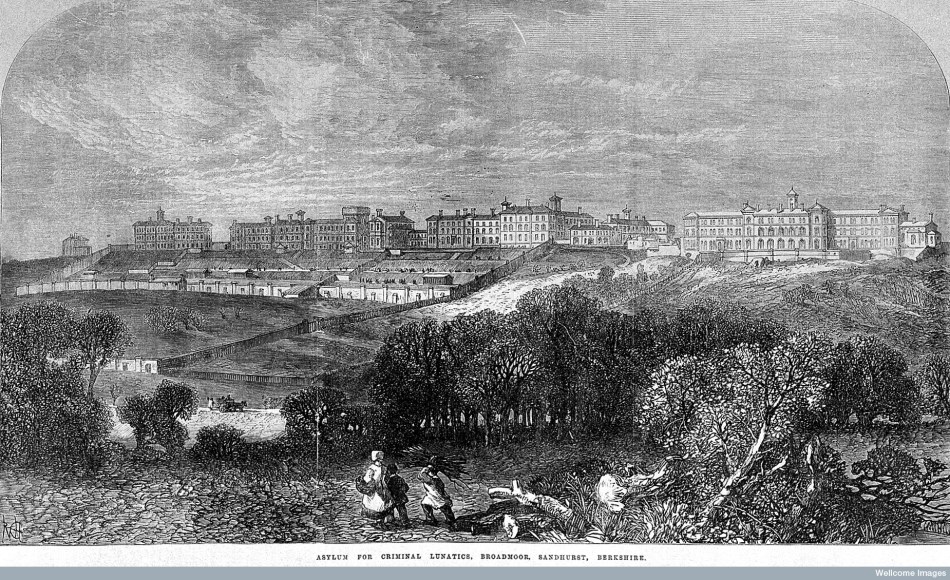
The Asylums Act of 1845 stipulated that each county had to have an asylum to cater for its pauper insane. These asylums were designed to resemble large country houses with landscaped gardens, and had ornamental drives, parkland, farms, cricket fields and estate walls. The airing courts attached to each accommodation block were designed so patients could view the vast landscape (fresh air and exercise also being part of treatment), and moral treatment was implemented. Contemporaries viewed moral treatment in terms of progress, but twentieth and twenty-first century scholars have criticized it. French philosopher Michel Foucault argued that asylums were institutions of social control within which physical chains were replaced with surveillance and coercion,[3] and historian Andrew Scull suggested that moral treatment was designed “to transform the lunatic” into “the bourgeois ideal of the rational individual.” Since then, other historians have shown that some asylum patients were expected to display “normative standards of behaviour,” which were usually gendered (along bourgeois lines) before they could be discharged.[4] It’s argued that moral treatment was designed to encourage traits such as temperance, industry, self-control, rationality and decorum in patients. Current and ongoing scholarly research suggests that this wasn’t the case in all asylums, though, and that some patients were discharged even though they did not possess these attributes.[5]
Asylums provided refuge and respite for some individuals struggling to survive in the world; in particular for those whose mental health issues fractured or destroyed their relationships with friends and families.
Historians (and contemporaries) agree that moral treatment failed. Asylums had limited resources with which to implement their extravagant claims of a cure and, from the 1860s, the existence of long-term chronic patients led to a rapid growth in the county asylum population; this meant that moral treatment was difficult to implement. Increasing patient numbers also led to the belief that insanity was incurable.[6] Such ideas led to the reintroduction of mechanical restraint and seclusion in some asylums, although asylum medical officers did manage to “find a compromise between sifting out and treating a minority, while managing large numbers of the chronically disordered.”[7]
It cannot be denied that there was a lot wrong with how insanity was conceptualized and treated in the nineteenth century. Treatment was sometimes cruel, isolating and degrading. Some asylums were poorly maintained, and there were institutions within which care and compassion were lacking. However, such spaces provided refuge and respite for some individuals struggling to survive in the world; in particular for those whose mental health issues fractured or destroyed their relationships with friends and families.
While writing my recent article on the treatment and experience of criminal lunatics in late-nineteenth century Broadmoor, I was surprised by the vast number of patients who, in their correspondence (to family members, friends, asylum doctors and other patients), described the positive impact asylum treatment was having on their health. Feeling alone and neglected by his family, one patient told another: “I am very glad and cheered when I hear the flute.”[8] The Broadmoor letters reminded me of scholar Barbara Taylor’s account of her time at Friern hospital (formerly Colney Hatch Asylum) in the 1980s. Taylor viewed Friern as a “sanctuary”: “I entered on my knees. I could no longer do ordinary life, and giving up the struggle was an incalculable relief.”[9]
Broadmoor patients’ accounts of asylum life and Taylor’s recollections are, in some instances, more than one hundred years apart, and yet the similarities are striking. Broadmoor features in some patients’ letters as a safe space for patients; they could work without fearing the repercussions of unemployment, or without the added pressure of knowing they had to provide for their families. Some patients’ friends and families also viewed Broadmoor as a place in which patients were restored to health. The friend of one patient wrote to the superintendent: “[you] have solved the problem of how to help and relieve [patients] without…destroying their self-respect.”[10]
Broadmoor was not only a place of recovery and respite, but also one where patients could forge friendships with other individuals.
Broadmoor was not only a place of recovery and respite, but also one where patients could forge friendships with other individuals. The development and maintenance of friendship (and survival) networks was seemingly crucial for some of Broadmoor’s patients, just as it was for patients in other asylums and hospitals. Taylor recalled how, in the 1980s, “the friendship of other patients…made my days tolerable.” She concluded that while institutional care was flawed, it “nurtured communities” crucial for patients’ wellbeing.[11]
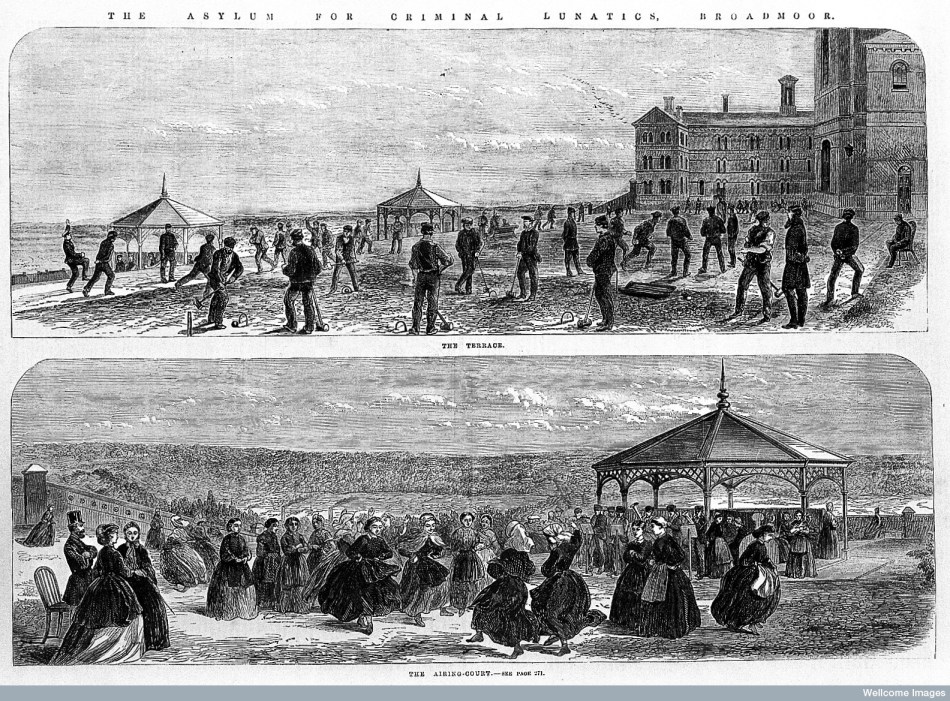
We see this at Victorian Broadmoor, too, where both male and female patients made friends, and where there was ample opportunity for relationships to develop. The recreational activities that were provided as part of treatment in Victorian asylums encouraged patients to interact with one another. Some male patients played team sports such as cricket, and female patients would take group rides and walks around the asylum’s grounds. The asylum’s blocks all had dayrooms where patients could play a variety of games, and where they could write, paint, sew, and read alongside each other while in conversation.
Patient Anthony Owston spent time talking to William Minor about “his soul” and Henry Dodwell wrote letters to another patient detailing his grievances and describing his sadness.[12] After receiving no correspondence from his family, Philip Dawe presumed they had given up on him: “to them I am probably long sensed lapsed [sic] into too hopeless imbecility or insanity to maintain a correspondence.”[13] He asked the superintendent if he could visit another patient in a different part of the asylum, presumably after meeting him at work or in the chapel. As with Longmore, whose letter began this essay, Dawe exemplifies being torn between his family and friends outside the asylum, and the doctors and patients inside the asylum. What is different, though, is the gulf that seemingly arose between Dawe and his family as a result of his mental illness; he perceived that they did not understand the reality of his condition. This was certainly one of the potential downsides of institutionalization. The rupture between Dawe and his loved ones did, however, seemingly encourage and strengthen his bonds with other patients. His case was not unusual.
While undertaking my research, it became clear that for some patients their insanity and absence from the home created a chasm between themselves and their loved ones who did not fully understand the struggles they faced. As a result, many received few or no visitors or letters. Their fellow patients could understand their illness and the isolation of being institutionalized, though, and the friendships that formed ensured survival, and for some happiness and contentment, at the asylum; as Taylor wrote, “friendship trumped madness – and this in itself could be a form of healing.”[14]
One of the things we can learn from patients’ accounts of institutionalized care in the nineteenth and twentieth centuries, then, is this: friendships and a sense of community can make a world of difference to the lives of people living with mental illness. The friendships some patients forged in asylums were vital in providing them with a sense of belonging. Friendships could relieve feelings of hopelessness that sometimes followed institutionalization, and could help to reduce the amount of time patients spent dwelling on their ill health and (in some cases) indefinite institutionalization. That patients could form relationships with people who could understand and accept them was particularly important if they had no one else to turn to, as in Dawe’s case.
The treatment of mental illness simply isn’t good enough.
I don’t want to romanticize this. We shouldn’t forget that institutionalized care was massively flawed, and that not all asylum patients made friends or adapted to being detained for an indefinite period of time away from their families and friends. Nor were all patients treated with dignity or “cured.” That said, the friendships formed within these institutions, and the structured treatment regime, were perceived positively by some patients, and made a difference to their lives. Today, there are no such institutions to care for the mentally ill; they have been replaced with day centers, overstretched hospital wards or prison cells, and—in some areas—Cognitive Behavioral Therapy (CBT) delivered over the telephone. The treatment of mental illness simply isn’t good enough.
Of course, the demise of the asylum isn’t necessarily a bad thing, but the services designed to replace institutionalized care do not always provide a sense of sanctuary to those living with mental illness. Moreover, the loneliness that accompanies ill mental health can be terrible. Some asylum patients managed to relieve feelings of isolation and despondency through their interactions with other patients, and thus the benefits of, and need for, community in the treatment of mental illness is clear. It’s a tragedy that the social activities that encouraged friendships and communities to develop between patients in the nineteenth and twentieth centuries aren’t as plentiful today. Despite well-meaning campaigns designed to reduce the shame associated with mental illness some stigma still exists, but without the community or specialized institutional care that seemingly benefited patients such as George Longmore or Philip Dawe in the nineteenth century, and Barbara Taylor in the twentieth century.
 Jade Shepherd is a historian of Victorian asylums, crime, masculinity and psychiatry at the University of Lincoln, UK. She completed her Ph.D at Queen Mary University of London in 2013, where she also taught history for five years. Her thesis, ‘Victorian Madmen: Broadmoor, Masculinity and the Experiences of the Criminally Insane 1863-1900’, examined the crimes, trials and asylum experiences of men committed into Broadmoor Criminal Lunatic Asylum. She’s currently working on a monograph, Broadmoor’s Men: Masculinity, Class and the Victorian Criminal Lunatic Asylum, and a number of small research projects: feigning insanity in Victorian prisons and asylums; wrongful confinement in county and criminal asylums; family life and the Victorian criminal asylum; and the treatment of the ‘criminal’ in Victorian prisons and asylums.
Jade Shepherd is a historian of Victorian asylums, crime, masculinity and psychiatry at the University of Lincoln, UK. She completed her Ph.D at Queen Mary University of London in 2013, where she also taught history for five years. Her thesis, ‘Victorian Madmen: Broadmoor, Masculinity and the Experiences of the Criminally Insane 1863-1900’, examined the crimes, trials and asylum experiences of men committed into Broadmoor Criminal Lunatic Asylum. She’s currently working on a monograph, Broadmoor’s Men: Masculinity, Class and the Victorian Criminal Lunatic Asylum, and a number of small research projects: feigning insanity in Victorian prisons and asylums; wrongful confinement in county and criminal asylums; family life and the Victorian criminal asylum; and the treatment of the ‘criminal’ in Victorian prisons and asylums.
* * *
Our collected volume of essays, Demand the Impossible: Essays in History As Activism, is now available on Amazon! Based on research first featured on The Activist History Review, the twelve essays in this volume examine the role of history in shaping ongoing debates over monuments, racism, clean energy, health care, poverty, and the Democratic Party. Together they show the ways that the issues of today are historical expressions of power that continue to shape the present. Also, be sure to review our book on Goodreads and join our Goodreads group to receive notifications about upcoming promotions and book discussions for Demand the Impossible!
* * *
We here at The Activist History Review are always working to expand and develop our mission, vision, and goals for the future. These efforts sometimes necessitate a budget slightly larger than our own pockets. If you have enjoyed reading the content we host here on the site, please consider donating to our cause.
![]()
Notes
[1] Individuals sent to Broadmoor were treated like any other asylum patient; it did not matter that they had committed a crime. They were patients, not criminals.
[2] Berkshire Record Office (BRO), D/H14/D2/2/1/1212/26.
[3] Michel Foucault, History of Madness, trans. by John Murphy and Jean Khalfa (London and New York: Routledge, 2006), p. 485
[4] Hide, Gender and Class, p. 143; Pamela Michael, ‘Class, gender and insanity in nineteenth-century Wales’, in Jonathan Andrews and Anne Digby (eds), Sex and Seclusion, Class and Custody: Perspectives on Gender and Class in the History of British and Irish Psychiatry (New York: Rodopi, 2004), pp. 95–122, 111–5.
[5] Jade Shepherd, ‘I am very glad and cheered when I hear the flute: The Treatment of Criminal Lunatics in Late Victorian Broadmoor’, Medical History, 4 (2016), 473-491, 485-488
[6] For example, J.K. Walton, ‘Casting out and bringing back in Victorian England: pauper lunatics, 1840–70’, in William F. Bynum, Roy Porter and Michael Shepherd (eds), The Anatomy of Madness: Essays in the History of Psychiatry 3 vols (London: Routledge, 1985–88), VII (1985), pp. 132–146, 142; Steven Cherry, Mental Health Care in Modern England: The Norfolk Lunatic Asylum/St Andrews Hospital 1810–1998 (Woodbridge: Boydell Press, 2003), pp. 89–90.
[7] Louise Hide, Gender and Class in English Asylums, 1890–1914 (Basingstoke: Palgrave Macmillan, 2014), p. 39
[8] Ibid., p. 481.
[9] Barbara Taylor, ‘The Demise of the Asylum in Late-Twentieth Century Britain: A Personal History’, Transactions of the Royal Historical Society, 21 (2011), 193-215, 212.
[10] Shepherd, ‘I am very glad and cheered when I hear the flute’, p. 481.
[11] Taylor, ‘The Demise of the Asylum’, pp. 213. 215.
[12] Jade Shepherd, ‘Victorian Madmen: Broadmoor, Masculinity and the Experiences of the Criminally Insane, 1863–1900’ (unpublished PhD thesis, Queen Mary University of London, 2013), p. 85.
[13] Ibid.
[14] Barbara Taylor, The Last Asylum: A Memoir of Madness in our Times (Penguin, 2014), p. 148.


I am a reader of Michel Foucault, and your analysis don’t surprise me.
Thanks for this good work.
LikeLiked by 1 person
This was really interesting! I had only heard horror stories about Victorian Asylums, so it was great to hear that there was a different side
LikeLiked by 1 person
Pingback: The Olmstead Decision and Community Mental Health – The Activist History Review
Pingback: Top 10 Dark Facts About Alice In Wonderland – Dailynews Journal
Pingback: Top 10 Dark Facts About Alice In Wonderland - article
Pingback: Top 10 Dark Facts About Alice In Wonderland